
MAC: How Anesthetic Potency is Defined
MAC-awake vs. MAC-intubation, and the Patient Factors That Shift the Curve
Pharmacokinetics · Volatile Agents · Anesthetic Potency · Dose-Response
Background:
Minimum Alveolar Concentration (MAC): the end-tidal concentration of an inhaled anesthetic that prevents purposeful movement to a standardized surgical stimulus in 50% of unpremeditated subjects. It can be described as a percentage, or as the MAC unit.
- MAC as a percentage of inspired/alveolar gas — this is the original, literal definition. Sevoflurane’s MAC is 2.0% because at sea level (760 mmHg), you need 2.0% of the gas mixture in the alveoli to be sevoflurane vapor to keep half of patients still.
- MAC as a multiplier (a “MAC unit”) — clinically, people often say things like “run at 1.0 MAC” or “we’re at 1.3 MAC.” Here MAC is being used as a normalized dose unit 1.0 MAC of sevoflurane (= 2.0%)
This was a concept first introduced by Dr. Ted Eger in 1965, to this day it remains the standard measure of anesthetic potency.
Potency:
More potent anesthetic require a lower MAC. And even though “alveolar concentration” sounds like a pharmacokinetic measurement, MAC really is a pharmacodynamic endpoint. The alveolar number is just what we can easily measure; what we actually care about is the drug’s effect at the spinal cord, where volatile agents block movement.
The standardized 1 MAC can be achieved via the following alveolar concentrations:
- 2.0% for sevoflurane
- 1.15% for isoflurane
- 6.0% for desflurane
- 104% for nitrous oxide
From this list we can see that isoflurane is incredibly potent, compared to nitrous oxide which is physiologically impossible to reach a MAC of 1.
Dosage:
MAC is not a single endpoint but a group of clinically distinct concentrations, each indexing a different physiologic response.

- MAC-awake (~0.3–0.5 MAC): the concentration at which 50% of patients are responsive=to verbal command, it is light sedation.
- MAC (1.0): 50 % of patients are unresponsive to skin incision etc. Surgical sedation.
- MAC-intubation, (~1.3 – 3 MAC): is the concentration that allows smooth laryngoscopy without coughing, bucking, or movement in 50% of patients.
- MAC-BAR (~1.5–2.0 MAC) blocks the autonomic and adrenergic response (tachycardia, hypertension) to incision in 50% of patients. Noted as being useful when surgical stimulation might destabilize a fragile patient
The observed MAC hierarchy isn’t arbitrary, it has physiological basis that is supported by evolutionary biology. It traces a rostral-to-caudal gradient down the nervous system. Cortical centers (where consciousness is) get knocked out first, at the lowest concentrations. Spinal motor pathways (where movement comes from) need more drug to suppress. And laryngeal/airway reflexes sit higher still. Your body is aware that it cannot breath if there is something in your throat doesn’t and it’ll defend that path (via gag reflex) even when the cortex is already offline.

The wide gap between MAC and MAC-EI in adults — roughly 1.0 vs. 3.0 with sevo alone — is the entire reason balanced anesthesia exists. If you tried to push the volatile high enough to intubate on its own, you’d tank the patient’s blood pressure long before you got there. So instead we add opioids (which slash MAC requirements through synergy) and a paralytic (which removes the muscular response entirely), and intubate at a much lower, hemodynamically friendlier volatile concentration.

Opioid-MAC reduction: the synergistic interaction between fentanyl-class opioids and volatile agents, where modest opioid doses produce disproportionately large reductions in MAC requirement.
In Practice:
MAC is not a fixed property of the drug it is a moving target shaped heavily by the patient.
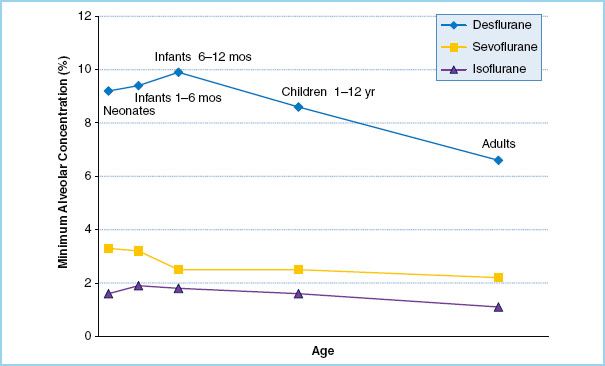
Age is the single most consistent modifier: MAC peaks in infants around 6 months of age, then declines roughly 6% per decade thereafter in a log-linear fashion across all volatile agents. This is why modern anesthesia machines accept the patient’s age as an input and display an age-corrected MAC; without it, the machine defaults to a 40-year-old reference and over-doses the elderly.
Temperature shifts MAC roughly 5% per degree Celsius — hypothermia potentiates volatile anesthesia, hyperthermia antagonizes it.
Opioid co-administration is synergistic rather than additive: a fentanyl infusion producing modest analgesic effect can reduce sevoflurane MAC by 50% or more, and remifentanil exhibits an even steeper reduction curve. This synergy is the pharmacologic foundation of balanced anesthesia — the reason a clinical sevoflurane concentration of ~1.0–1.5% is sufficient for major surgery despite a stated MAC of 2.0%.
Other significant modifiers include pregnancy (↓~30%), acute alcohol or benzodiazepine intoxication (↓), chronic alcohol use (↑), hypernatremia (↑), hyponatremia (↓), and acute amphetamine or cocaine use (↑).
Limitations
It is worth keeping the limits of MAC in mind. By definition at MAC 1, half of the patients will move to incision, this is why clinical practice typically targets a 1.2–1.3 MAC for surgical anesthesia to push the dose-response curve closer to 95%.
MAC also does not predict awareness — movement and consciousness are not always correlated, a paralyzed patient at adequate MAC for immobility may still be inadequately hypnotized and vice versa; this is the rationale for processed-EEG monitors like BIS as a complementary input.
Finally, MAC by itself does not fully capture the synergy with intravenous medications: the end-tidal volatile concentration on the monitor is only one variable in the pharmacodynamic equation when opioids, propofol, ketamine, or dexmedetomidine are running in parallel.
In practice, MAC is best understood as a calibration point, not a number to chase, rather a reference against which the rest of the anesthetic technique is titrated.
Leave a Reply